The Utah State Hospital (USH) is an Institution for Mental Disease (IMD) that complements the local mental health centers by providing specialized services not available in community settings. The hospital's population includes adults and children for whom no appropriate, less restrictive environment is currently available. Various services are provided for four groups of people: 1) pediatric services for children and adolescents, 2) forensic services for those found not guilty of crimes by reason of insanity, guilty and mentally ill, or not competent to proceed with court actions, 3) adult services for adults who are civilly committed, and 4) Acute Recovery Treatment Unit (ARTC) for acute care of adults from four rural mental health centers: Central Utah MHC, Four Corners MHC, Northern Counseling Center, and San Juan MHC.
Additional information regarding the Utah State Hospital can be found on its official website found at: Utah State Hospital
During the 2015 General Session, the Legislature appropriated for Fiscal Year 2016, $59,342,600 from all sources for State Hospital. This is a 5.4 percent increase from Fiscal Year 2015 revised estimated amounts from all sources. The total includes $43,263,400 from the General/Education Funds, an increase of 4.1 percent from revised Fiscal Year 2015 estimates.
In addition to statewide compensation and internal service fund cost increases, the following appropriation adjustments were made during the 2015 General Session:
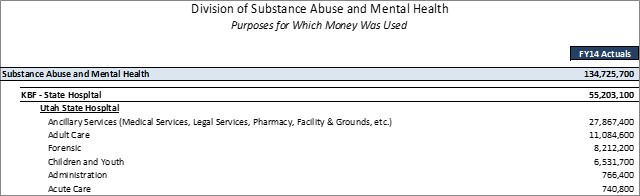
For the most recent completed fiscal year, the following information represents the purposes for which the money was used:
Beds in both adult and pediatric civil units at the State Hospital are distributed based upon formulas established in statute (UCA 62A-15-611 and 612) which reflect "the percentage of the state's . . . population located within a mental health catchment area" and several other smaller mitigating factors. The Forensic units at the State Hospital are considered statewide programs as well. However, the funding for forensic units is not distributed based upon a formula. Instead, "all the money comes to the State Hospital and serves patients statewide as determined by the judges."
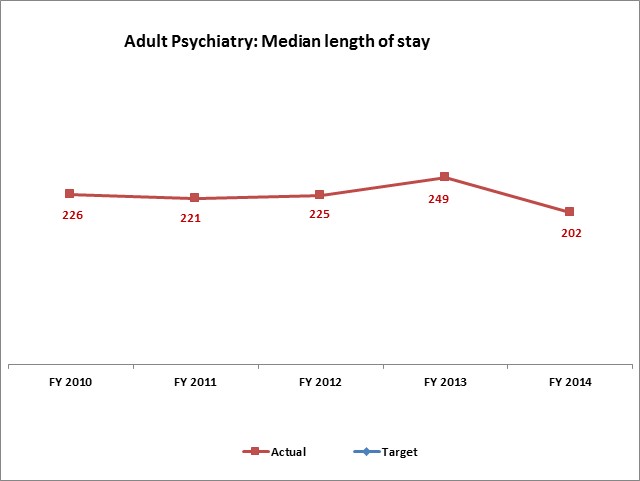
Regarding the positive trend greater than 5% in the adult population median length of stay (LOS) from the state hospital performance measure, the hospital states, "Variation depends upon patient acuity and barriers in discharge planning identified by treatment team and LMHA's. Severity of illness for patients admitted is not equal across the board and can vary from year to year. 2013 increase LOS could be a result of closing 30 beds in 2012 as lower acuity patients were released . . . Though measuring Length of Stay has to take into consideration the impact of many variables (i.e., housing availability, patient clinical acuity, finance and benefit approvals, and other discharge barriers); it is a valuable indicator in monitoring systemic efficiencies and trends. 2013 USH increase LOS for Adult patients could have been the result of closing 30 beds in 2012 as lower acuity patients were released. USH does track other outcome measures that are specific to our clinical care such as BPRS and SOQ which are included in other reports. LOS was chosen and has been tracked as part of the COBI for quite some time inasmuch as it is still seen as a valuable systems indicator. Though measuring Length of Stay has to take into consideration the impact of many variables (i.e., housing availability, patient clinical acuity, finance and benefit approvals, and other discharge barriers); it is a valuable indicator in monitoring systemic efficiencies and trends. 2013 USH increase LOS for Adult patients could have been the result of closing 30 beds in 2012 as lower acuity patients were released. USH does track other outcome measures that are specific to our clinical care such as BPRS and SOQ which are included in other reports. LOS was chosen and has been tracked as part of the COBI for quite some time inasmuch as it is still seen as a valuable systems indicator . . . Though measuring Length of Stay has to take into consideration the impact of many variables (i.e., housing availability, patient clinical acuity, finance and benefit approvals, and other discharge barriers); it is a valuable indicator in monitoring systemic efficiencies and trends. 2013 USH increase LOS for Adult patients could have been the result of closing 30 beds in 2012 as lower acuity patients were released. USH does track other outcome measures that are specific to our clinical care such as BPRS and SOQ which are included in other reports. LOS was chosen and has been tracked as part of the COBI for quite some time inasmuch as it is still seen as a valuable systems indicator."
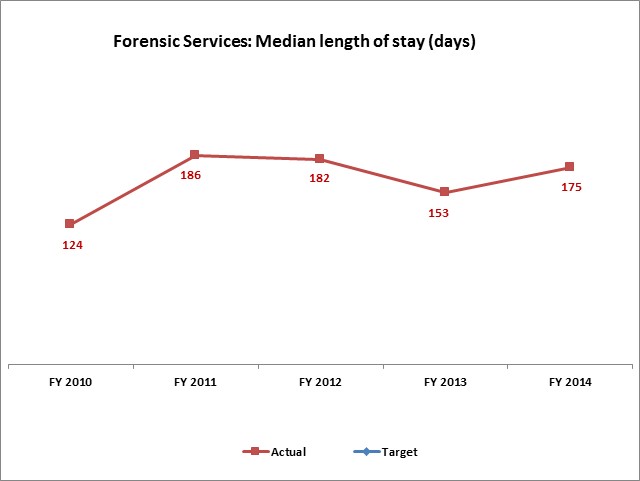
Regarding the negative trend greater than 5% in the forensic population median length of stay (LOS) from the state hospital performance measure, the hospital states, "Variation depends upon patient acuity, coordination with district courts, patient competency restoration, etc."
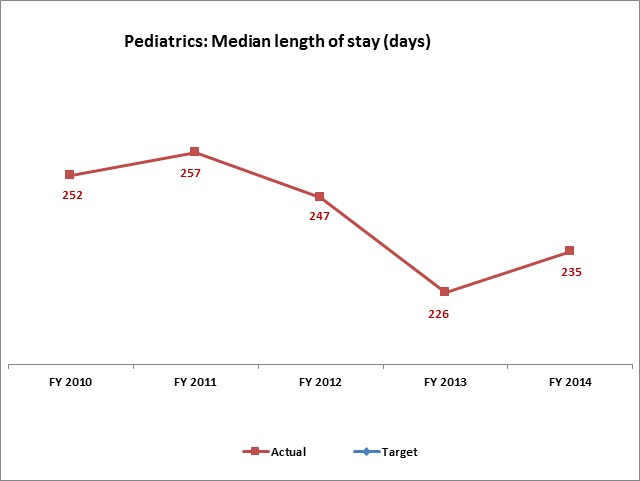
Regarding the positive trend greater than 5% in the pediatric population median length of stay (LOS) from the state hospital performance measure, the hospital states, "Variation depends upon patient acuity and barriers in discharge planning identified by treatment team and LMHA's. Overall trend with length of stay is improving over the past 8 years."
Most adult patients in the Utah State Hospital are not eligible for Medicaid funding because of regulations associated with the federal Omnibus Reconciliation Act (OBRA) of 1987. These regulations define any nursing facility with 40 percent or more mentally ill residents as an IMD and then prohibit Medicaid funding for residents between the ages of 22 and 65 living in an IMD.
Adult services provide 152 beds to the community mental health centers as prescribed by state statute. Pediatric services provides 72 beds to the community mental health centers as prescribed by state statute. The beds available for use by the local mental health centers are allocated according to population. UCA 62A-15-611 governs the adult allocation and UCA 62A-15-612 governs the pediatric allocation. The statute indicates that as the state population changes, the distribution of beds available to the local authorities should be reviewed and reallocated.
COBI contains unaudited data as presented to the Legislature by state agencies at the time of publication. For audited financial data see the State of Utah's Comprehensive Annual Financial Reports.