Medicaid is a joint federal/state entitlement service consisting of three programs that provide health care to selected low-income populations: (1) a health insurance program for low-income parents (mostly mothers) and children; (2) a long-term care program for the elderly; and (3) a services program to people with disabilities. Overall, Medicaid is an "optional" program, one that a state can elect to offer; however, if a state offers the program, it must abide by strict federal regulations. It also becomes an entitlement program for qualified individuals; that is, anyone who meets specific eligibility criteria is "entitled" to Medicaid services. The federal government establishes and monitors certain requirements concerning funding, and establishes standards for quality and scope of medical services. Medicaid includes requirements to provide certain services and to serve specific populations. States may expand their program to cover additional "optional" services and/or "optional" populations. In addition, states have some flexibility in determining certain aspects of their own programs in the areas of eligibility, reimbursement rates, benefits, and service delivery. As long as services meet State and federal standards, the federal government will provide a match for all State money spent on Medicaid. The match is known as the Federal Medical Assistance Percentage (FMAP). The entire Medicaid program is based upon an approved contract with the federal government, known as the State Plan. The federal government must approve all changes and/or amendments to the State Plan. If the State were to provide a service without federal approval, then the State would pay 100% of the costs rather than the usual federal match.
During the 2015 General Session, the Legislature appropriated for Fiscal Year 2016, $1,487,594,700 from all sources for Medicaid Mandatory Services. This is a 4.8 percent increase from Fiscal Year 2015 revised estimated amounts from all sources. The total includes $305,854,100 from the General/Education Funds, an increase of 6 percent from revised Fiscal Year 2015 estimates.
In addition to statewide compensation and internal service fund cost increases, the following appropriation adjustments were made during the 2015 General Session:
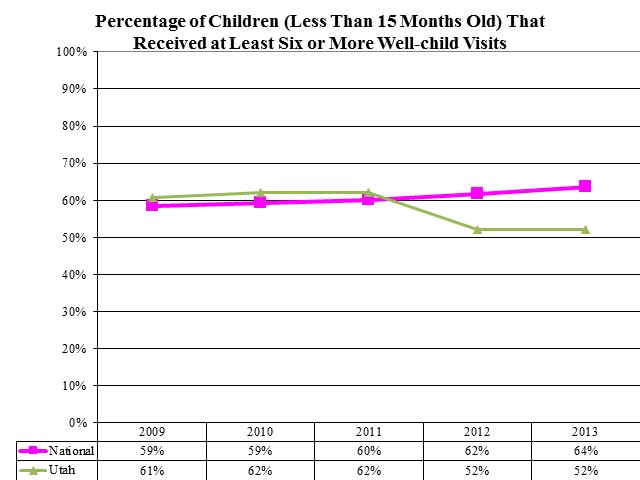
Percentage of Children (Less Than 15 Months Old) That Received at Least Six or More Well-child Visits
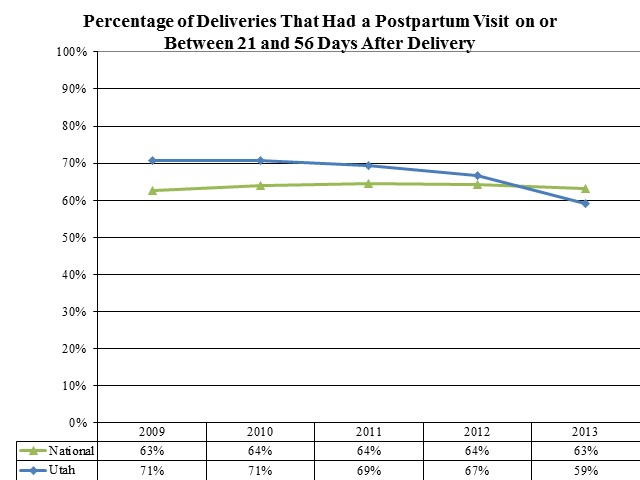
Percentage of Deliveries That Had a Postpartum Visit on or Between 21 and 56 Days After Delivery
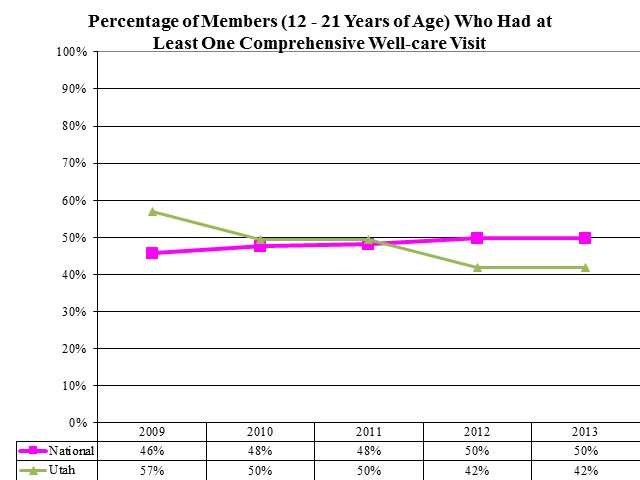
Percentage of Members (12 - 21 Years of Age) Who Had at Least One Comprehensive Well-care Visit
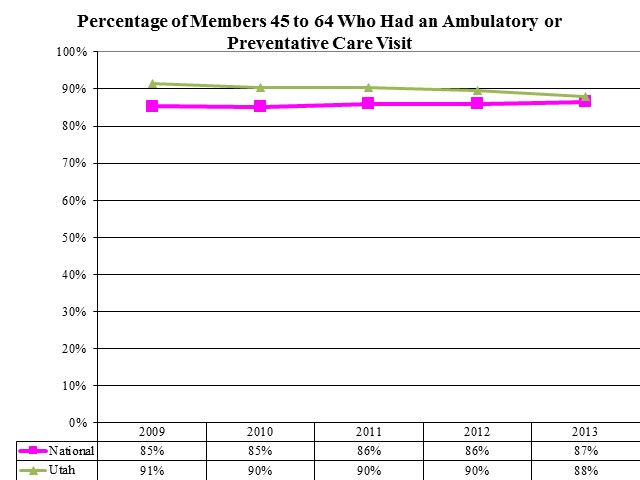
Percentage of Members 45 to 64 Who Had an Ambulatory or Preventative Care Visit
Most providers for Medicaid must meet Medicare provider requirements to receive reimbursement for serving Medicaid clients. Additionally, they must accept Medicaid reimbursement as payment in full. The provider may charge the patient for services not covered by Medicaid only when the provider has advised the patient in advance that Medicaid does not cover the services and the patient has agreed in writing to pay for the services. Medicaid does not pay for any services not considered medically necessary.
The client's Medicaid Identification Card will state when a co-pay is required and for what type of service. Pregnant women and children are not subject to the co-pay requirement. The provider is responsible to collect the co-pay at the time of service or bill the client. The total amount paid to the provider reflects the amount of the client's co-pay. For a list of co-pays by service please visit http://health.utah.gov/umb/forms/pdf/adultcomp.pdf.
There are currently 57 services included in the entire Medicaid Program. Of these, inpatient hospital, outpatient hospital, intermediate care facilities for individuals with intellectual disabilities, long-term care, physician, dental, pharmacy, and health maintenance organizations make up over 75 percent of all Medicaid expenditures. Medicaid services in Utah are in two budgetary line items: Medicaid Mandatory Services and Medicaid Optional Services. The line dividing mandatory and optional services is occasionally blurred by the fact that some optional services are mandatory for specific populations or in specific settings. For example, the federal government requires more services for children and pregnant women. Additionally, clients in institutionalized settings receive a wider range of services. The State's flexibility includes federal waivers that allow some latitude in program implementation, as well as to offer some additional optional services.
Mandatory services in the Medicaid Program come from decisions by the federal government regarding required services. These include: inpatient and outpatient hospital, physician services, skilled and intermediate care nursing facilities, medical transportation, home health, nurse midwife, pregnancy-related services, lab and radiology, kidney dialysis, Early Periodic Screening Diagnosis and Treatment, and special reimbursement to community and rural health centers. The federal government requires the State to pay Medicare premiums and co-insurance deductibles for aged, blind, and disabled persons with incomes up to 100 percent of the Federal Poverty Level. Additionally, the State pays for Medicare premiums for two other groups of qualifying individuals: (1) those with incomes up to 120 percent of the Federal Poverty Level and (2) and those with incomes between 121 and 135 percent of the Federal Poverty Level.
There are nine budget programs within the Medicaid Mandatory Services line item, which include: Inpatient Hospital, Contracted Health Plans, Nursing Home, Outpatient Hospital, Physician Services, Other Mandatory Services, Crossover Services, Medical Supplies, and State-run Primary Care Case Management.
The Early Periodic Screening Diagnosis and Treatment Program, called Child Health Evaluation and Care in Utah, is a mandatory federal program which requires the State to screen all Medicaid children up to age 21 at scheduled intervals. The mandate includes providing all medically necessary services, such as organ transplants or any other service needed, regardless of cost or if it is normally covered by Medicaid. Utah's 12 local health departments provide the federally-required education and outreach for this program.
The State has designated five major population groupings that may receive health care from the Medicaid Program. These include: (1) aged - the elderly or disabled who receive federal Supplemental Security Income (SSI) and persons in nursing facilities (grouped together as aged), (2) blind and disabled individuals, (3) children who receive Temporary Assistance for Needy Families (TANF) benefits, or are in the Foster Care program, (4) TANF adults with dependent children, and (5) pregnant women. Each of these groups is discussed in more detail later in this section.
Aged
Individuals aged 65 and over qualify for Medicaid if they qualify for SSI, which provides an income of approximately 77.6 percent of the Federal Poverty Level (FPL). They also qualify for food stamps. Many of the elderly also qualify for Medicare coverage. The Medicaid Program pays for the premiums and deductibles for those eligible under both programs. Medicare pays the actual medical cost for most of these people. Medicaid is also required to pay Medicare premiums, co-insurance, and deductibles for anyone qualifying for Medicare who has income up to 100 percent of FPL, but only has to pay Medicare premiums for those between 100 and 135 percent of FPL.
Medicaid also covers non-SSI aged people whose income does not exceed 100 percent of FPL. Aged people with income over 100 percent of FPL can spend down to the Medically Needy Income Limit (100% of FPL) to receive Medicaid.
Blind and Disabled
Persons with disabilities are eligible for services under the Medicaid Program. The criteria for disability require that a person be unable to participate in gainful activity for at least a year, or have a medical condition that will result in death. Among the disabilities covered are mental retardation, blindness, mental health, spinal injury, and AIDS. Income is limited to 100 percent of the Federal Poverty Level. There is an asset limit of $3,000 for families. The asset limit does not include a primary residence or a car. Eligible individuals also qualify for food stamps.
Children
Aid to Families with Dependent Children (AFDC) was a joint federal-state program which provided financial assistance to families with children deprived of the support of at least one parent. In 1996, AFDC was replaced with block grants to the states and the Temporary Assistance to Needy Families (TANF). In general, people who meet AFDC eligibility criteria that were in effect on July 16, 1996 are eligible for Medicaid. Also, those people who qualify for a TANF grant may be eligible for Medicaid.
The Medically Needy Children program is for children who do not qualify for assistance under normal Family Medicaid because they still have the support of a parent. The family may spend down to become eligible. This is an optional group not required by the federal government. Many children previously eligible for the Medically Needy Children program have become eligible in the mandatory programs for children.
In addition to the previously mentioned TANF children, there are three groups of children covered under the Medicaid Program. These are: (1) medically needy children, (2) children up to age 18 with family income up to 133 percent of the Federal Poverty Level (FPL), and (3) children in subsidized adoptions.
There is no asset test for children applying for Medicaid.
Children in Foster Care are eligible for Medicaid coverage if they meet Medicaid Program requirements. The State is responsible for their medical care. Most children placed in foster care have histories of abuse or neglect. Often there are unresolved medical and mental health problems. Each year, a number of children come into the custody of the State and are placed for adoption. Some of these children have serious medical problems which makes them hard to place. In some of these cases, the State subsidizes the adoption. Some families receive a small stipend to assist in the cost of care for these children, and the State covers the child's medical care under Medicaid until the child is 18 years old. Children that age out of foster care, regardless of income and assets, receive Medicaid services until they turn 26 through the Independent Living Program, unless they are eligible for another Medicaid program.
TANF Adults
The group referred to as TANF Adults includes those adults with dependent children who are either categorically or medically needy and meet the basic program requirements. Some of the individuals may need to "spend down" to obtain Medicaid services, which means that they must reduce their disposable income with payments to Medicaid or with medical bills which they have incurred.
There are two groups of people who qualify for Medicaid under the TANF Program. These include: (1) those in the basic program where a child lacks the support of one parent, and (2) those in two-parent families that qualify under the unemployed parent program. The majority of eligible families are deprived because of divorce, desertion, or unwed mothers. TANF families may also qualify for food stamps. Depending on family size, the TANF grant and food stamps provide an income between 62 and 74 percent of the Federal Poverty Level.
In addition to the basic Family Employment Program (FEP), there is also a program for unemployed two-parent families. This program provides cash assistance for seven months in any 13-month period. One parent in families in this program is required to work 32 hours a week (in an emergency work program) and spend at least 8 hours per week seeking regular employment. With the exception of the time limitation and work requirement, the criteria and benefits for the Family Employment Program - Two Parent are the same as those for the regular FEP. Federal law requires that the family be eligible for Medicaid for the full 12 months of the year. Besides those eligible through FEP cash assistance, there are several programs which provide transitional Medicaid coverage for periods of 4 months (for child support-related eligibles) or 24 months (for people who no longer receive cash assistance due to child support payments or earnings).
Pregnant Women
The prenatal/pregnancy program helps pregnant women receive prenatal care. The program covers the mother from the time of application to 60 days after the birth. A woman only needs to meet the eligibility requirements in any one month to be eligible for the balance of the pregnancy. Children born to women on this program are eligible for Medicaid (after the first 60 days) for the rest of the first year under the postnatal program.
Because of the Department's budget reorganization in FY 2011, some of the detail between FY 2010 and FY 2011 nonlapsing balances does not tie out by line item. For analysis of current budget requests and discussion of issues related to this budget click here.
The source of finance entitled "Transfers - Medicaid - UDC" is for state match from the Department of Corrections for Medicaid-eligible inmates who receive hospital inpatient services.
COBI contains unaudited data as presented to the Legislature by state agencies at the time of publication. For audited financial data see the State of Utah's Comprehensive Annual Financial Reports.